




Ko ngā whati o te tibial plateau me ngā whati o te tibial shaft ipsilateral e kitea whānuitia ana i roto i ngā whara kaha-nui, ā, 54% he whati tuwhera. Kua kitea e ngā rangahau o mua ko te 8.4% o ngā whati o te tibial plateau e hono ana ki ngā whati o te tibial shaft i te wā kotahi, ko te 3.2% ia o ngā tūroro whati o te tibial shaft he whati tibial plateau i te wā kotahi. He mārama ehara i te mea onge te whakakotahitanga o ngā whati o te tibial plateau ipsilateral me te shaft.
Nā te kaha o te kaha o ēnei whara, he maha ngā wā ka kino rawa ngā kiko ngohengohe. I roto i te ariā, he pai ngā painga o te pūnaha pereti me te tīwiri ki te whakau ā-roto mō ngā whati papatahi, engari he mea whakaaroaro hoki mēnā ka taea e te kiko ngohengohe o te rohe te aro atu ki te whakau ā-roto me te pūnaha pereti me te tīwiri. Nō reira, e rua ngā kōwhiringa e whakamahia whānuitia ana mō te whakau ā-roto o ngā whati papatahi tibial me ngā whati kakau tibial:
1. Tikanga MIPPO (Minmally Invasive Plate Osteosynthesis) me te pereti roa;
2. Whao intramedullary + tīwiri papatahi.
E rua ngā kōwhiringa kua kōrerotia i roto i ngā tuhinga, engari kāore anō kia whakaaetia i tēnei wā ko tēhea te mea pai ake, te mea iti iho rānei, e pā ana ki te tere whakaora whati, te roa whakaora whati, te tūnga o ngā peka o raro, me ngā raruraru. Hei whakatika i tēnei, i whakahaerehia e ngā tohunga o tētahi hōhipera whare wānanga o Korea tētahi rangahau whakatairite.

I roto i te rangahau, e 48 ngā tūroro i whara te tibial plateau me ngā whati o te tibial shaft. I roto i ēnei, e 35 ngā kēhi i rongoatia ki te tikanga MIPPO, me te whakaurunga taha o te pereti maitai hei whakapiri, ā, e 13 ngā kēhi i rongoatia ki ngā tīwiri plateau me te huarahi infrapatellar mō te whakapiri whao intramedullary.
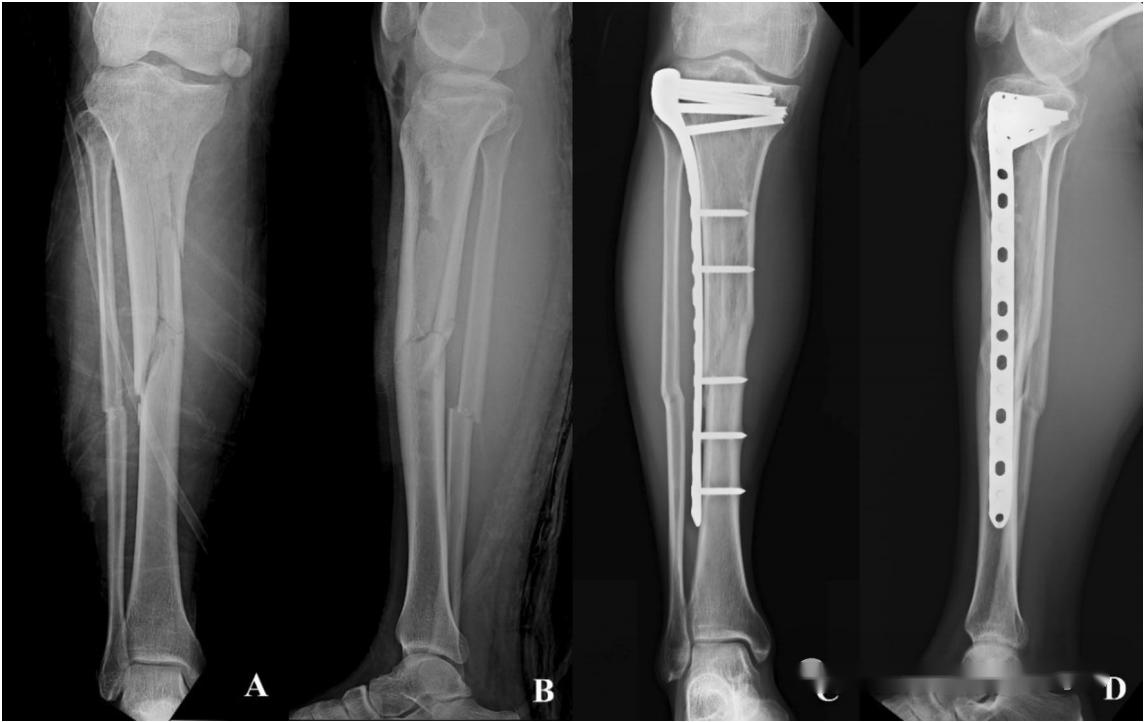
▲ Take 1: Te whakapiri ā-roto o te pereti maitai MIPPO taha. I puta mai tētahi tāne 42-tau te pakeke, i uru ki tētahi aituā motuka, me te whati tuwhera o te kakau tibial (momo Gustilo II) me te whati kōpeketanga o te papa tibial medial plateau i te taha (momo Schatzker IV).
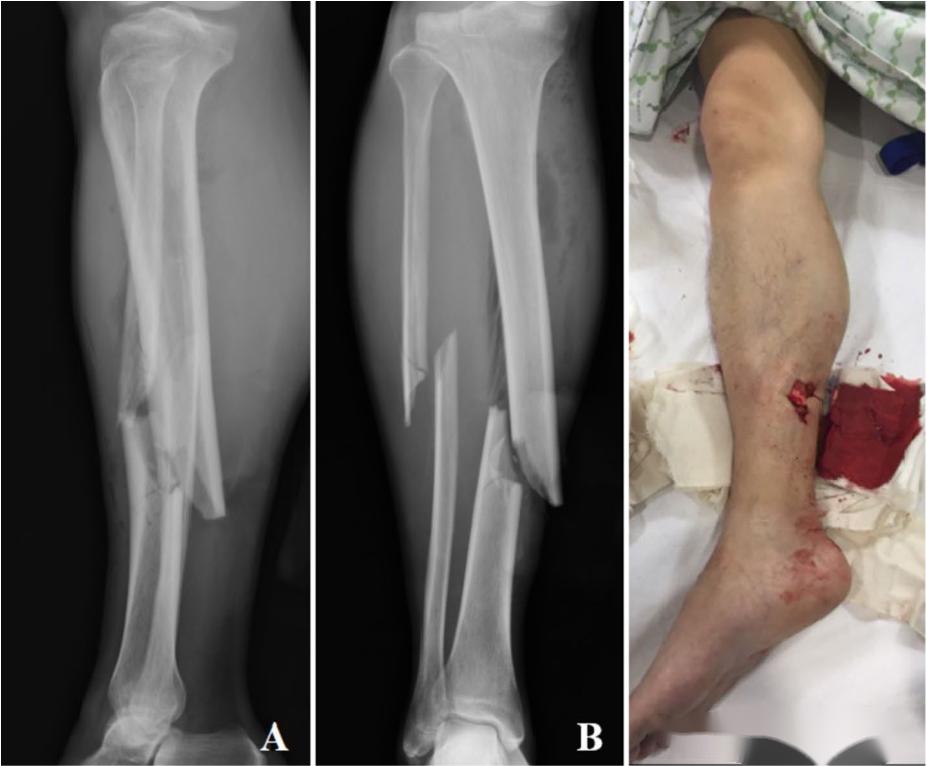
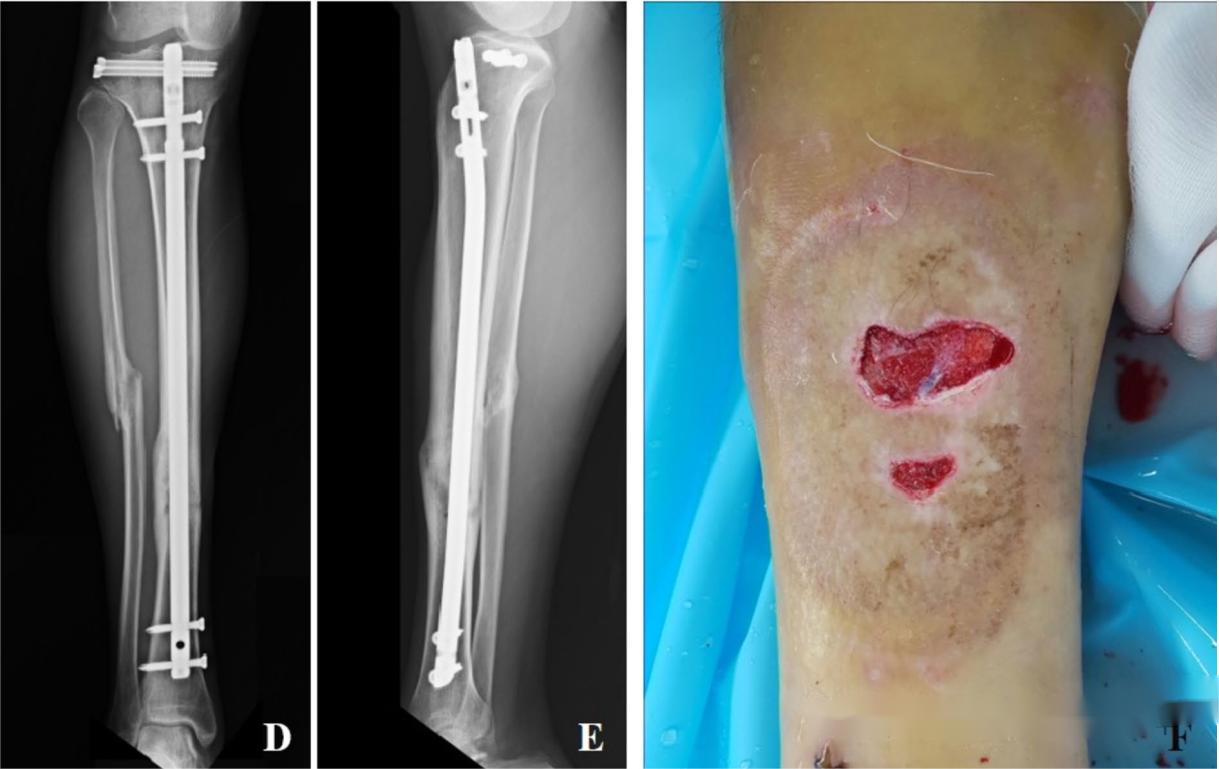
▲ Take 2: Tīwiri papatahi tibial + whakapiringa whao ā-roto suprapatellar intramedullary. I puta mai tētahi tāne 31-tau te pakeke, i uru ki tētahi aituā motuka, me te whati tuwhera o te kakau tibial (momo Gustilo IIIa) me te whati papatahi tibial lateral i te taha (momo Schatzker I). Whai muri i te tango i te pakaru o te patunga me te rongoā patunga pēhanga kino (VSD), i honoa te patunga ki te kiri. E rua ngā tīwiri 6.5mm i whakamahia hei whakaiti me te whakapiringa o te papatahi, ā, i muri mai ko te whakapiringa whao intramedullary o te kakau tibial mā te huarahi suprapatellar.
E whakaatu ana ngā hua kāore he rerekētanga nui ā-tatauranga i waenga i ngā tikanga pokanga e rua e pā ana ki te roa o te whakaora whati, te tere whakaora whati, te tūnga o te waewae o raro, me ngā raruraru.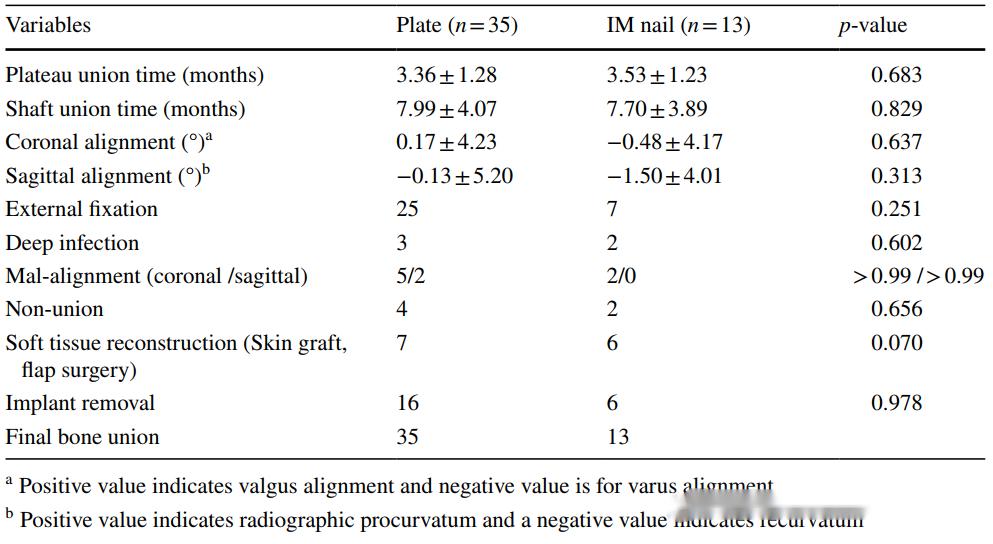
He rite ki te huinga o ngā whati o te kakau tibial me ngā whati o te hononga pona, ngā whati rānei o te kakau femur me ngā whati o te kaki femur, ka taea hoki e ngā whati o te kakau tibial i puta mai i te kaha nui te arahi ki ngā whara i te hononga turi e tata ana. I roto i te mahi haumanu, ko te aukati i te tātaritanga hē te mea nui i roto i te tātaritanga me te maimoatanga. Hei tāpiri, i roto i te whiriwhiri i ngā tikanga whakapiri, ahakoa e kī ana ngā rangahau o nāianei kāore he rerekētanga nui, he maha tonu ngā mea hei whakaaroaro:
1. Mēnā he uaua te whakapiri i te tīwiri ki ngā whati o te tibial plateau kua pakaru, me whakamahi pea i tētahi pereti roa me te whakapiri MIPPO hei whakau i te tibial plateau, hei whakaora i te ōritetanga o te mata o te hononga me te tūnga tika o te peka o raro.
2. Mēnā he whati ngāwari o te tibial plateau, i raro i ngā tapahi iti rawa te whakaekenga, ka taea te whakatutuki i te whakaiti whai hua me te whakapiri i ngā tīwiri. I roto i ēnei āhuatanga, ka taea te tuku i te kaupapa matua ki te whakapiri tīwiri, ā, muri iho ko te whakapiri i ngā whao suprapatellar intramedullary o te kakau tibial.
Wā tuku: Maehe-09-2024





